Chronic Kidney Disease (CKD) and diabetes mellitus are two health conditions intricately linked, with the latter being a leading cause of renal impairment worldwide. Elevated urinary albumin-to-creatinine ratio (UACR) serves as a key biomarker indicating worsening kidney function and predicting adverse cardiovascular outcomes in diabetic patients. Managing UACR effectively is vital because persistent albuminuria not only signals ongoing renal damage but also correlates with increased mortality risk.
Recent research outcomes reinforce the growing consensus that a combination, or dual therapy, approach targeting multiple pathways offers superior benefits compared to traditional monotherapy. This approach targets the underlying mechanisms driving kidney damage, leading to better reduction in UACR and potentially delaying the progression to end-stage renal disease (ESRD). Let’s delve deeper into how dual therapy is revolutionizing the management of CKD in diabetic patients.
Why Is UACR Reduction a Priority?
UACR is a widely used marker to assess kidney health, especially in diabetic populations. Elevated UACR indicates increased permeability of the glomerular filtration barrier, signaling early nephropathy. Persistent proteinuria not only signifies ongoing renal injury but also predisposes patients to cardiovascular complications, including hypertension and heart failure.
Traditionally, treatments focused on controlling blood pressure and blood glucose levels using medications like ACE inhibitors and ARBs. While these monotherapies have shown benefits, they often become insufficient over time, necessitating more comprehensive strategies to address the multifactorial nature of diabetic nephropathy.
The Evidence Supporting Dual Therapy
Superior Efficacy in UACR Reduction
Multiple recent studies have demonstrated that combining therapeutic agents yields better results in lowering UACR compared to using a single agent. For example, a recent article published by “Dual Therapy Outperforms Monotherapy for UACR Reduction in CKD and Diabetes” by Docwire News consolidates evidence across diverse patient cohorts indicating that dual therapy regimens consistently outperform monotherapy in reducing proteinuria levels. This is crucial because reducing UACR helps mitigate further renal deterioration and cardiovascular risks.
The Role of Finerenone in Renoprotection
Finerenone, a non-steroidal mineralocorticoid receptor antagonist, has emerged as a promising candidate in combination therapies. Research on its efficacy suggests that it can significantly reduce proteinuria even when patients are on maximum doses of other agents like dapagliflozin and telmisartan, which are part of standard care. The study available from (PDF) Evaluating the Efficacy of Finerenone in Reducing Proteinuria… highlights how finerenone adds a protective layer against renal inflammation and fibrosis, key processes in diabetic nephropathy.
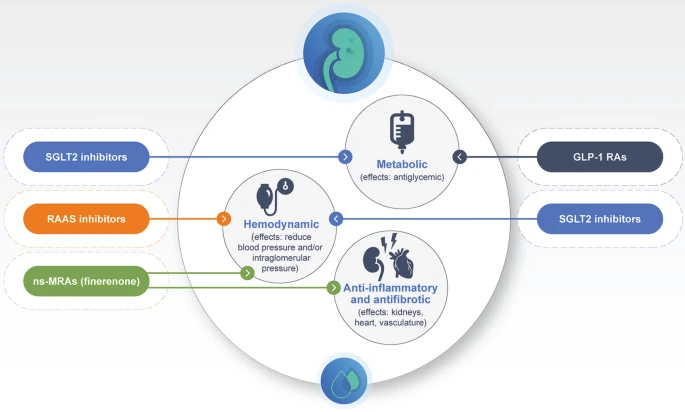
Why Combining Therapies Is More Effective
The pathogenesis of diabetic kidney disease is complex, involving hemodynamic changes, inflammation, fibrosis, and oxidative stress. Monotherapy often targets only one aspect, which limits its effectiveness. Dual therapy, on the other hand, can address multiple pathogenic processes simultaneously. For instance, utilizing SGLT2 inhibitors like dapagliflozin lowers glomerular hyperfiltration and reduces oxidative stress, whereas ARBs diminish intraglomerular hypertension and protein leakage.
In addition, some emerging therapies target mineralocorticoid receptors or inflammatory pathways, providing a multi-pronged approach that enhances overall renal protection. The combined effect has resulted in more significant and sustained UACR reductions, slowing disease progression.
Early Screening and Intervention: Key to Preventing Irreversible Damage
A compelling point raised by studies like the one on “40% of diabetics suffer from silent kidney damage”, underscores the importance of early detection through regular screening. Detecting microalbuminuria early allows timely initiation of combined therapies, which can significantly alter disease trajectories and prevent progression to ESRD.
Additional Strategies and Lifestyle Modifications
Beyond pharmacotherapy, lifestyle interventions play a critical role in managing CKD and diabetes. Patients are encouraged to maintain optimal blood glucose levels, control blood pressure, reduce salt intake, adopt a balanced diet rich in antioxidants, and engage in regular physical activity. These measures complement dual therapy regimens, providing a holistic approach to kidney health.
Conclusion: A Paradigm Shift in Managing CKD in Diabetic Patients
The evidence is increasingly clear—dual therapy approaches are more effective than monotherapy in reducing UACR and protecting kidney function in diabetic CKD patients. The integration of drugs like finerenone, SGLT2 inhibitors, and RAAS blockers offers a promising avenue to slow disease progression and improve quality of life. Healthcare providers must consider comprehensive treatment strategies tailored to individual patient profiles, emphasizing early detection and intervention.
As research continues to evolve, the emphasis on personalized medicine and combination therapies will likely become the standard of care. Patients equipped with early diagnoses and appropriate treatment plans can significantly decrease their risk of irreversible renal damage, ultimately leading to better health outcomes.
For more updated news please keep visiting Hourly Prime News.